Since 2017, India’s Tuberculosis (TB) programme has been undertaking active case finding (ACF) outside the healthcare settings among high-risk populations.
| Photo Credit: AP
Since 2017, India’s Tuberculosis (TB) programme has been undertaking active case finding (ACF) outside the healthcare settings among high-risk populations. Recently, a team led by the Chennai-based National Institute of Epidemiology (ICMR-NIE) undertook the first-ever national-level analysis to measure the quality of ACF. This study was commissioned by the Central TB Division. The results of the study were published on September 21 in the journal Global Health Action.
ACF data were available only for 657 districts. Of the three ACF cycles recommended among the high-risk populations each year, 642 districts (98%) undertook just one cycle. Most districts were not clear what constituted one ACF cycle.
An ACF cycle is mapping of the high-risk population and screening and testing them in a given period. “Based on a study in South Africa, two ACF cycles in a year appear to have additional benefits over one cycle. There is no evidence to suggest three cycles are needed,” Dr. Hemant Deepak Shewade, a senior scientist at ICMR-NIE and the first author of the paper, told The Hindu.
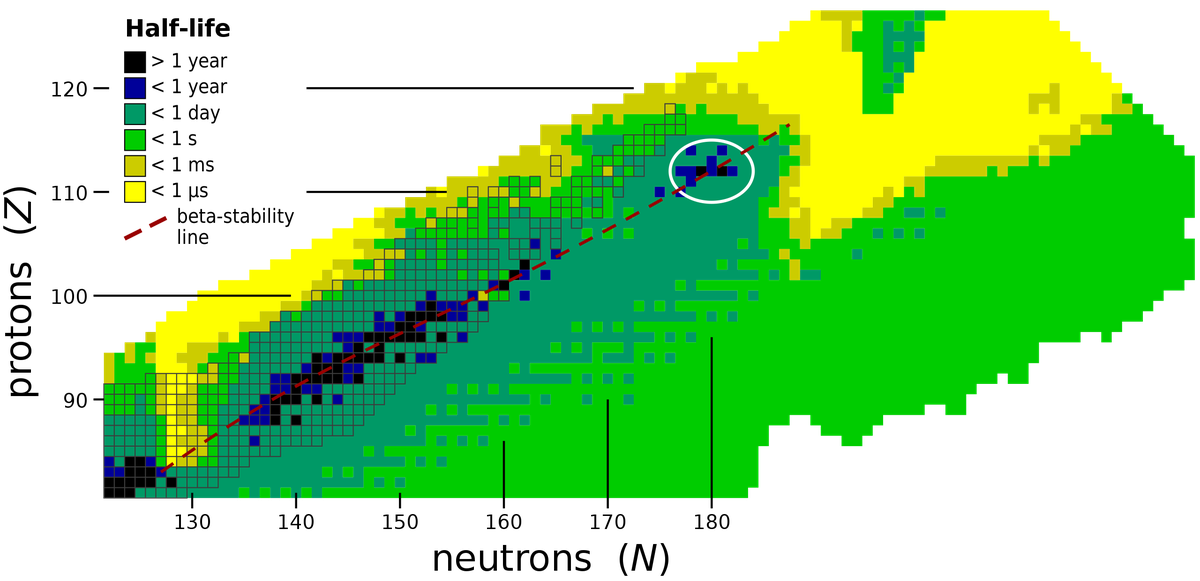
Based on the available data, the quality of ACF was measured using three indicators — screening at least 10% of the district population for TB, testing at least 4.75% of the screened, and diagnosing at least 5% TB among those tested. Alternative indicator (that is a composite measure of the latter two indicators) is the number of persons who must be screened to diagnose one active TB case or number needed to screen (NNS); NNS should be less than 1,538.
The study found that the quality of ACF was suboptimal across the country in 2021. Not one State met all the three ACF quality indicator cut-offs or the NNS. At the national level, 9.3% of the population were screened, just 1% of the screened were tested and 3.7% of the tested were diagnosed. The NNS was 2,824 which is much higher than 1,538.
Within a district, all high-risk populations are to be first identified (which is called mapping) and ACF should be conducted among them. But mapping was undertaken only in areas where ACF was conducted and not for the entire district. “We did not have comprehensive data on the number of high-risk populations in the district to report the extent of ACF among high-risk populations. Hence, we reported the extent of ACF among the district population and compared it against a derived cut-off of 10%,” he said.
They found that States that reported high percentage of screening had very low percentage of testing among the screened. Meanwhile, States that had low screening had high levels of testing and diagnosis. Quality ACF indicators for each State should be based on TB epidemiology in the State.
The percentage of people tested among the screened was the worst of the three indicators; it was even worse in the case of population-based screening. “This could be because sputum collection and transport was suboptimal or the presumptive TB cases were required to visit the nearest testing facilities on their own leading to attrition,” he said.
The recommendations of this study have the potential to guide India’s ACF guidance for TB.