




Photo used for representation purpose only.
| Photo Credit: The Hindu
In 2017, the Health Ministry and the Gujarat government covered up three Zika virus cases detected between November 2016 and February 2017. India informed the WHO about the outbreak in Gujarat only in May 2017, six months after the first case was detected. The news of the outbreak became known only when the WHO posted the information on its website. Eight years later, India has been found shying away from divulging all the details of a polio case detected in Meghalaya’s West Garo Hills district in early August this year.
On August 12, the ICMR-NIV Mumbai Unit, which is a WHO-accredited polio laboratory, confirmed that the polio case detected in Meghalaya was a type-1 vaccine-derived poliovirus (VDPV), and reported the results to the Union Health Ministry, the Meghalaya State government and the WHO, Dr Roderico H. Ofrin, WHO Representative to India, told The Hindu in an email. Yet, the first report of the polio case published by PTI two days later on August 14 called it a “suspected” case of polio. Based on unnamed officials, the PTI report from Shillong said: “A two-year-old boy in a remote village in Meghalaya’s West Garo Hills district has been found with symptoms of poliomyelitis or polio, prompting health authorities to start an investigation.” The report, which quoted a senior doctor at the Directorate of Health Services, further added that “a boy with symptoms of poliomyelitis was detected yesterday [August 13] during routine surveillance” even when the results were available on August 12.
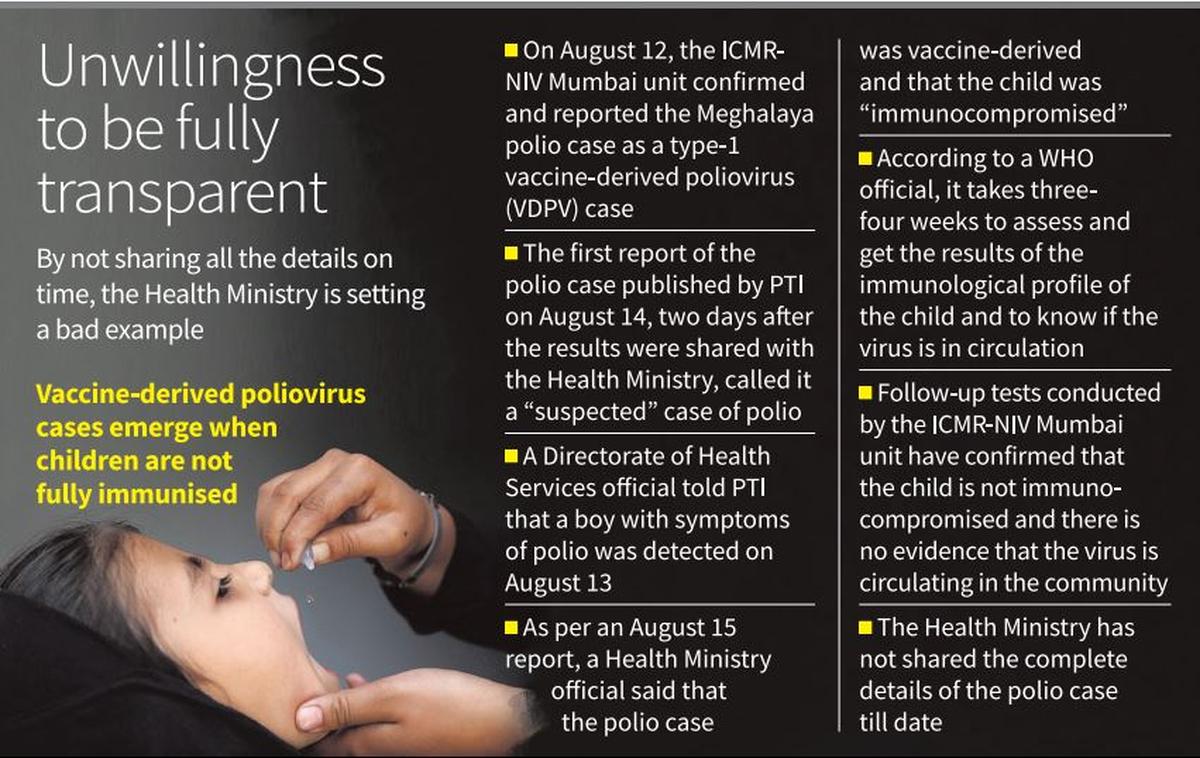
According to an August 15 report in The Hindustan Times, a Union Health Ministry official said that the polio case was vaccine-derived and that the child was “immunocompromised”. Vaccine-derived polio can be of two types — circulating vaccine-derived polio (cVDVP) or immunodeficiency related vaccine-derived poliovirus (iVDPV). In the case of iVDPV, the polio is caused in an immune-deficient individual. By saying that the child is “immuocompromised”, the official was suggesting that it was a case of iVDPV. In reality, on August 15, it was not known whether the child was immunocompromised. It finally turned out that the child was not immunocompromised, and therefore was not a case of iVDPV.
On August 20, a senior official from the Union Health Ministry told The Hindu that the Meghalaya case has been confirmed as being vaccine-derived polio, and ruled out wild type virus causing polio in the little child. However, on the same day, health officials in Meghalaya were ambiguous on whether it was vaccine-derived or caused by wild poliovirus. The State health officials said samples collected from the child were sent to ICMR-NIV’s Mumbai unit for testing, and the government was “awaiting the test results to ascertain if it is a case of wild poliovirus or a circulating vaccine-derived poliovirus”.
While the Union Health Ministry officials told The Hindu that the polio case was vaccine-derived, details about whether the virus belonged to type-1, type-2 or type-3 have not been revealed till date.
Dr. Ofrin’s email makes it clear that the Union Ministry officials and Meghalaya health officials were making conflicting and incorrect statements —whether the polio was vaccine-derived or caused by wild poliovirus, the date when the case was detected, insinuation by the State government officials that it might be a case of iVDPV, and refusal to divulge the details about poliovirus typing (type-1, type-2 or type-3) — despite being aware of the results, which were shared by the ICMR-NIV Mumbai Unit on August 12.
“The type 1 VDPV was confirmed and reported by ICMR-NIV Mumbai on August 12, 2024. It has been determined… that the polio case is not caused by the wild poliovirus type 1,” Dr. Ofrin told The Hindu by email on September 16. “The virus has been confirmed as type 1 VDPV by ICMR-NIV Mumbai as well as by CDC Atlanta. Both labs have confirmed that this is not an imported strain of type-2 VDPV or wild poliovirus type-1.”
Explaining the delay in confirming whether the vaccine-derived polio is due to circulating virus or due to immunodeficiency in the child, Dr. Ofrin said: “As per standard protocols laid down for responding to such isolations, immediate actions were initiated by the programme to assess the immunological profile of the child from whom the virus had been isolated and to also assess if there is any evidence of circulation of the virus in the community. It generally takes three-four weeks to complete the process and receive the results.”
According to Dr. Ofrin, the follow-up tests conducted by ICMR-NIV Mumbai have confirmed that the immunological profile of the child was normal and there was no evidence that the virus was circulating in the community. “The Ministry of Health and Family Welfare, the State government of Meghalaya, and WHO are fully aware of the details of the results,” he said.
Published – October 05, 2024 09:12 pm IST